“I really believe in the ‘Cali sober’ method. It’s helped me. I actually just hit five years clean.” Aaron Carter made that declaration on Adam Grandmaison’s “No Jumper” podcast — just days before he died on November 5, 2022. As he fingered a joint, he continued, “This, I don’t consider a drug. I consider this a gift from God.”
Attached is a list of medical articles that document medical warnings against marijuana that are running in newspapers throughout the country, to warn in advance of participation in 420 events.
Average flower is 17.1% in one state with legal sales of recreational marijuana, Colorado, much higher than the national average (HIDTA, 2017), and as high as 30% THC in some samples (NBC News report). It should be noted that variation in testing results is quite high between laboratories (Jikomes and Zoroob, 2018).
Jikomes N, Zoorob M. The Cannabinoid Content of Legal Cannabis in Washington State Varies Systematically Across Testing Facilities and Popular Consumer Products. Sci Rep. 2018 Mar 14;8(1):4519. doi: 10.1038/s41598-018-22755-2. https://www.nature.com/articles/s41598-018-22755-2.pdf
Processed cannabis reaches up to 90% THC
Jikomes N, Zoorob M. The Cannabinoid Content of Legal Cannabis in Washington State Varies Systematically Across Testing Facilities and Popular Consumer Products. Sci Rep. 2018 Mar 14;8(1):4519. doi: 10.1038/s41598-018-22755-2. https://www.nature.com/articles/s41598-018-22755-2.pdf
Marijuana is the Number 1 substance now found in Colorado suicides, 10-19 years old, 2014-2016
Causes mental illness, and is associated with onset of schizophrenia and other psychotic disorders such as bipolar disorder with psychosis
Association with schizophrenia and other psychotic disorders such as bipolar and schizophrenia. (Miller, 2017; Cougle et al., 2015), completed suicides and suicide attempts (Arendt et al., 2013; Silins et al., 2014; Clarke et al., 2014) and violence towards others (Arseneault et al., 2000; Dugre et al., 2017; Harford et al., 2018) particularly in those who develop marijuana-induced psychosis.
Arseneault L, Moffitt TE, Caspi A, Taylor PJ, Silva PA. Mental disorders and violence in a total birth cohort: results from the Dunedin Study. Arch Gen Psychiatry. 2000;57(10):979-86.
Arendt M, Munk-Jørgensen P, Sher L, Jensen SO. Mortality following treatment for cannabis use disorders: predictors and causes. J Subst Abuse Treat. 2013;44(4):400-6.
Clarke MC, Coughlan H, Harley M, Connor D, Power E, Lynch F, Fitzpatrick C, Cannon M. The impact of adolescent cannabis use, mood disorder and lack of education on attempted suicide in young adulthood. World Psychiatry. 2014;13(3):322-3.
Cougle JR et al. (2015). Quality of life and risk of psychiatric disorders among regular users of alcohol, nicotine, and cannabis: An analysis of the National Epidemiological Survey on Alcohol and Related Conditions (NESARC). J Psychiatr Res., 66-67, 135-141
Di Forti M, et al. Proportion of patients in South London with first-episode psychosis attributable to use of high potency cannabis: a case-control study. Lancet Psychiatry. 2015;2(3):233-8.
Harford TC, Chen CM, Kerridge BT, Grant BF. Self- and other-directed forms of violence and their relationship with lifetime DSM-5 psychiatric disorders: Results from the National Epidemiologic Survey on Alcohol Related Conditions-III (NESARC-III). Psychiatry Res. 2018;262:384-392.
Silins E, Horwood LJ, Patton GC, Fergusson DM, Olsson CA, Hutchinson DM, Spry E, Toumbourou JW, Degenhardt L, Swift W, Coffey C, Tait RJ, Letcher P, Copeland J, Mattick RP, for the Cannabis Cohorts Research Consortium. Young adult sequelae of adolescent cannabis use: an integrative analysis. Lancet Psychiatry 2014; 1(4): 245-318.
Starzer MSK, Nordentoft M, Hjorthøj C. (2018) Rates and Predictors of Conversion to Schizophrenia or Bipolar Disorder Following Substance-Induced Psychosis. Am J Psychiatry,175(4), 343-350
Harm to unborn, nursing babies
Marijuana harms unborn children (Jenkins et al., 2007; Trezza et al., 2012; Tortoriello et al., 2014; Grewen et al., 2015; Zumbrun et al., 2015; Leemaqz et al., 2016; Benevenuto et al., 2017), and may concentrate in breast milk if used repeatedly (Perez-Reyes and Wall, 1982; Grotenhermen, 2003), with consequences for the developing neonate (Astley and Little, 1990).
Astley SJ, Little RE. Maternal marijuana use during lactation and infant development at one year. Neurotoxicol Teratol. 1990 Mar-Apr;12(2):161-8.
Benevenuto SG et al., Recreational use of marijuana during pregnancy and negative gestational and fetal outcomes: An experimental study in mice. Toxicology. 2017 Feb 1;376:94-101
Grewen K, Salzwedel AP, Gao W. Functional Connectivity Disruption in Neonates with Prenatal Marijuana Exposure. Front Hum Neurosci. 2015;9:601.
Grotenhermen F. Pharmacokinetics and pharmacodynamics of cannabinoids. Clin Pharmacokinet. 2003;42(4):327-60. Review.
Jenkins KJ, Correa A, Feinstein JA, Botto L, Britt AE, Daniels SR, Elixson M, Warnes CA, Webb CL; American Heart Association Council on Cardiovascular Disease in the Young. Non-inherited risk factors and congenital cardiovascular defects: current knowledge: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young: endorsed by the American Academy of Pediatrics. Circulation. 2007 Jun 12;115(23):2995-3014.
Leemaqz SY et al. Maternal marijuana use has independent effects on risk for spontaneous preterm birth but not other common late pregnancy complications. Reprod Toxicol. 2016;62:77-86.
Perez-Reyes M, Wall ME. Presence of delta9-tetrahydrocannabinol in human milk. N Engl J Med. 1982;307(13):819-20.
Tortoriello G, et al. Miswiring the brain: Δ9-tetrahydrocannabinol disrupts cortical development by inducing an SCG10/stathmin-2 degradation pathway. EMBO J. 2014;33(7):668-85.
Trezza,V. et al. Altering endocannabinoid neurotransmission at critical developmental ages: impact on rodent emotionality and cognitive performance. Front Behav Neurosci. 2012; 6: 02. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3265033/
Zumbrun EE et al. Epigenetic Regulation of Immunological Alterations Following Prenatal Exposure to Marijuana Cannabinoids and its Long Term Consequences in Offspring. J Neuroimmune Pharmacol. 2015; 10(2):245-54.
Marijuana causes cyclic vomiting
Sorensen CJ, DeSanto K, Borgelt L, Phillips KT, Monte AA. Cannabinoid Hyperemesis Syndrome: Diagnosis, Pathophysiology, and Treatment-a Systematic Review. J Med Toxicol. 2017;13(1):71-87. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5330965/
Alaniz VI, Liss J, Metz TD, Stickrath E. Cannabinoid hyperemesis syndrome: a cause of refractory nausea and vomiting in pregnancy. Obstet Gynecol. 2015 Jun;125(6):1484-6.
Marijuana can trigger violence in those with PTSD and make PTSD worse
Wilkinson ST, Stefanovics E, Rosenheck RA. Marijuana use is associated with worse outcomes in symptom severity and violent behavior in patients with posttraumatic stress disorder. J Clin Psychiatry. 2015 Sep;76(9):1174-80.
Friedman A, Glassman K, Terras A Violent Behavior as Related to Marijuana and Other Drugs, by Albert Journal of Addictive Diseases, Vol 20(1), 2001,pp. 49-72. Marijuana users nearly as likely to engage in violent behaviors as crack users.
Marijuana is linked to increased driving fatalities
Staples JA, Redelmeier, DA, The April 20 Cannabis Celebration and Fatal Traffic Crashes in the United States. JAMA Intern Med. 2018;178(4):569-572. doi:10.1001/jamainternmed.2017.8298 Rate of traffic fatalities go up 12% after 4/20 festivities, in comparison to one week before and one week after.
Bosker WM, Kuypers KP, Theunissen EL, et al. Medicinal Δ9-tetrahydrocannabinol (dronabinol) impairs on-the-road driving performance of occasional and heavy cannabis users but is not detected in standard field sobriety tests. Addiction. 2012;107(10):1837-1844.
Compton WN, Volkow Nd, Lopez MF. Medical marijuana laws and cannabis use: intersections of health and policy, JAMA Psychiatry. 2017: 74 (6): 559-560
Del Balzo G, Gottardo R, Mengozzi S, Dorizzi RM, Bortolotti F, Appolonova S, Tagliaro F, “Positive” urine testing for Cannabis is associated with increased risk of traffic crashes, Journal of Pharmaceutical and Biomedical Analysis. https://doi.org/10.1016/j.jpba.2017.12.059
Ramaekers JG, Kauert G, van Ruitenbeek P, Theunissen EL, Schneider E and Manfred R Moeller, High-Potency Marijuana Impairs Executive Function and Inhibitory Motor Control. Amer Col of Neuropsychopharmacology (2006) 31, 2296–2303.
Raemakers, JG Driving Under the Influence of Cannabis: An Increasing Public Health Concern. JAMA published online March 26, 2018 Regular cannabis users wrongfully believe that cannabis does not affect their driving performance or that they can compensate for cannabis-associated impairment. Raemakers_2018 JAMA driving editorial.pdf
World Health Organization. Drug Use and Road Safety: A Policy Brief. Geneva, Switzerland: World Health Organization; 2016.
Marijuana associated with lung disease, cancer
Marijuana smoke is associated with lung disease (Tan et al., 2009; Tashkin, 2015) and the development of some cancers (Efird et al., 2004; Lackson et al., 2012). High levels of the cannabinoid receptor that is preferentially activated by THC (CB1) correspond to shorter survival in many cancers (Michalski et al., 2008; Carpi et al., 2015; Suk et al., 2016)
Carpi S, Fogli S, Polini B, Montagnani V, Podestà A, Breschi MC, Romanini A, Stecca B, Nieri P. Tumor-promoting effects of cannabinoid receptor type 1 in human melanoma cells. Toxicol In Vitro. 2017 Apr;40:272-279. doi: 10.1016/j.tiv.2017.01.018. Epub 2017 Jan 26
Efird JT, Friedman GD, Sidney S, Klatsky A, Habel LA, Udaltsova NV, Van den Eeden S, Nelson LM. The risk for malignant primary adult-onset glioma in a large, multiethnic, managed-care cohort: cigarette smoking and other lifestyle behaviors. J Neurooncol. 2004 May;68(1):57-69.
Lackson et al., 2012, Population-based case-control study of recreational drug use and testis cancer risk confirms an association between marijuana use and nonseminoma risk. Cancer 188:5374-83
Michalski CW, Oti FE, Erkan M, Sauliunaite D, Bergmann F, Pacher P, Batkai S, Müller MW, Giese NA, Friess H, Kleeff J. Cannabinoids in pancreatic cancer: correlation with survival and pain. Int J Cancer. 2008;122(4):742-50. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2225529/pdf/nihms38106.pdf
Suk KT, Mederacke I, Gwak GY, Cho SW, Adeyemi A, Friedman R, Schwabe RF. Opposite roles of cannabinoid receptors 1 and 2 in hepatocarcinogenesis. Gut. 2016;65(10):1721-32. http://gut.bmj.com/content/gutjnl/65/10/1721.full.pdf
Tan WC, et al. Marijuana and chronic obstructive lung disease: a population-based study. CMAJ. 2009;180(8):814-20
Tashkin DP. The respiratory health benefits of quitting cannabis use. Eur Respir J. 2015;46(1):1-4
Legal marijuana increases youth use (Cerda et al., 2017) and is associated with youth switching to more potent marijuana products (Borodovsky et al., 2017)
Use by youth in 8th and 10th grades has gone up significantly in Washington State (Cerda et al., JAMA Pediatrics ). School districts with the highest density of legal dispensaries in Colorado have a 30% higher rate of use in students by the time they reach their senior year of high school (Healthy Kids Colorado Survey, 2015: Adolescent Health); and to compile data on density of dispensaries for each school district https://weedmaps.com/dispensaries/in/united-states/colorado)
The percentage of youth on probation testing positive for marijuana has increased steadily since 2012 (DPS, 2017)
Borodovsky JT, Lee DC, Crosier BS, Gabrielli JL, Sargent JD, Budney AJ. U.S. cannabis legalization and use of vaping and edible products among youth. Drug Alcohol Depend. 2017; 177:299-306. https://www.ncbi.nlm.nih.gov/pubmed/28662974
Cerdá M, Wall M, Feng T, Keyes KM, Sarvet A, Schulenberg J, O’Malley PM, Pacula RL, Galea S, Hasin DS. Association of State Recreational Marijuana Laws With Adolescent Marijuana Use. JAMA Pediatr. 2017;171(2):142-149. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5365078/
Marijuana decreases IQ in those who begin their use young
Meier MH, Caspi A, Ambler A, Harrington H, Houts R, Keefe RS, McDonald K, Ward A, Poulton R, Moffitt TE. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A. 2012 Oct 2;109(40):E2657-64. doi: 10.1073/pnas.1206820109
Mj harms developing adolescent and young adult brains.
Camchong J, Lim KO, Kumra S. Adverse Effects of Cannabis on Adolescent Brain Development: A Longitudinal Study. Cereb Cortex. 2017 Mar 1;27(3):1922-1930. doi: 10.1093/cercor/bhw015. https://academic.oup.com/cercor/article/27/3/1922/3056289
Allan GM Simplified guideline for prescribing medical cannabinoids in primary care Canadian Family Physicians Vol 64: February 2018 2018 Cannabis Prescribing Guidelines.pdf.
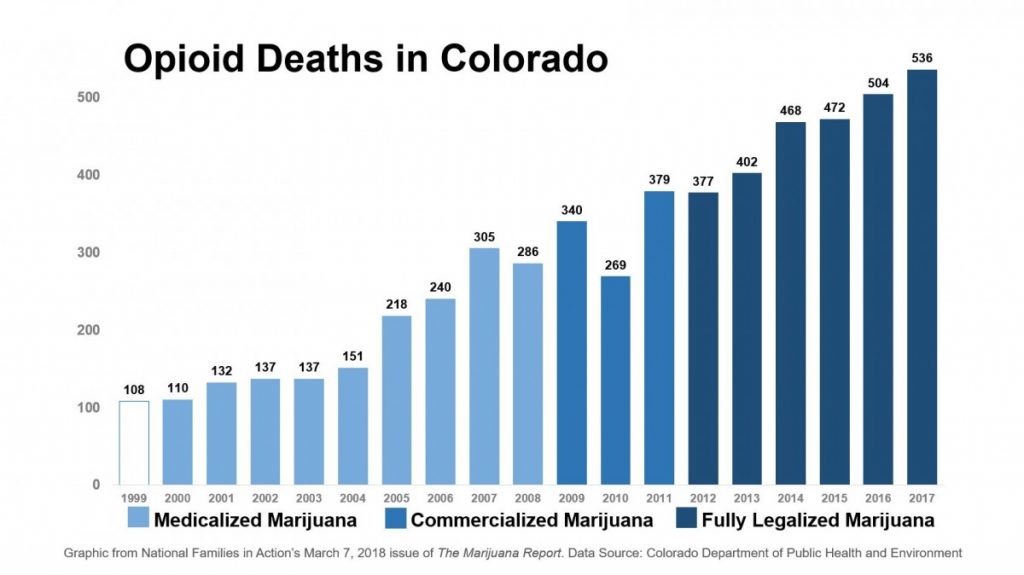
Olfson M, Wall M Cannabis Use and Risk of Prescription Opioid Use Disorder in the United States American J Psychiatry. Cannabis use, even among adults with moderate to severe pain, was associated with a substantially increased risk of nonmedical prescription opioid use at 3-year follow-up. https://doi-org.proxy.hsi.ucdenver.edu/10.1176/appi.ajp.2017.17040413
Graph provided by The Marijuana Report/National Families in Action. March 2018
Olfson M, Wall M Cannabis Use and Risk of Prescription Opioid Use Disorder in the United States, American J Psychiatry. Cannabis use, even among adults with moderate to severe pain, was associated with a substantially increased risk of nonmedical prescription opioid use at 3-year follow-up. https://doi-org.proxy.hsi.ucdenver.edu/10.1176/appi.ajp.2017.17040413
Practicing psychiatry is very tricky. Heavy-duty pills have serious side effects. To some observers, psychiatric medications are prescribed only to make money and psychiatrists are seen as evil witches casting spells. The world is not so simple, as there are psychiatrists working to get patients off medications.
A number of websites such as Mad in America and Beyond Meds channel gripes against Psychiatry and its medications. At the same time, there’s been a flood of people suffering from mental health and addiction problems in need of treatment. Forbes Magazine recently reported that there’s a shortage of psychiatrists in the USA.
Politics of Mental Health Treatment
We suspect that veterans with PTSD* and marijuana use are promoting the increased demand for psychiatrists. Back in 2005, SAMSHA and ONDCP tried to warn Americans that teen marijuana use can introduce mental health problems in those with no previous issues. The DSM manual, which is like a Bible for Psychiatry, gives guidelines for diagnosing and treating symptoms.
Parents Opposed to Pot recommends staying free from marijuana and other drug abuse as the best defense against having a psychiatric condition. The turbo-charged marijuana of today puts a far greater number of people at risk than the weaker pot of the ‘70s. In Colorado and Washington, dispensaries sell marijuana that averages 22 to 28% THC, compared to 1-4% back in hippy days.
Changes in HIPAA Law could put more checks and balances on Psychiatry. Because of HIPAA Law, families are not allowed to know enough. An ideal system of mental health treatment would pull together families and psychiatrists and patients. When Representative Murphy introduced a mental health care reform bill two years ago, many people supported it because it promised to change HIPAA. However, the ACLU and patients’ rights groups fought this provision and a bill passed the House without making this crucial change.
Psychiatric Practices and System Called into Question
Often insurance will not pay for optimal addiction treatment unless there is an underlying mental health diagnosis. Even when there is a mental health diagnosis, treatment also fails if patients are released from hospitals prematurely.
The Washington Post reports of a Maryland mother who suffocated two children after she was released from a psychiatric hospital too soon. This unfortunate woman, Sonya Spoon, had suffered from abandonment at four months age, lived in orphanages and suffered from a head injury at age 18. Her adoptive mother had warned the doctors against releasing her from the hospital too early, before an antidepressant could take effect.
Despite complete failure in the mental health care system, the criminal justice system sentenced her to 45 years in prison. It is tragedy on so many levels for both her and the two toddlers she killed. Unfortunately, the prison system is filled with both addicts and those suffering from untreated mental health disorders.
Beginning in the Kennedy Administration, a movement to de-institutionalize mental health patients began. Psychiatry hoped that medications could replace institutions. Pharmaceutical companies jumped at the opportunity, produced new drugs and marketed them vigorously. It would be nice if “magic pills” really did work all the time, but they often cause additional problems and outlive their usefulness.
Everyone admits there are failures in the mental health care system, and many of Psychiatry’s critics want to eliminate all pills and forced treatments. However, plenty of people believe psychiatric pills help them. (Please see comments below by Jane Thompson whose medications bring relief to Bipolar Disorder.) To think all psychiatric medications are worthless is like thinking all mental illness develops because the parents are evil. Amateurs should never tell others not to take their psychiatric meds.
Psychiatry Lags Behind Other Branches of Medicine
Some branches of medicine, such as those that treat cancer and heart disease, have made great strides in the past century. Unfortunately, Psychiatry has not. Many doctors besides psychiatrists are known to . Books by Robert Whitaker, Joanna Moncrieff, MD and others call into question the overuse of psychiatric drugs. Whitaker’s Anatomy of an Epidemic, 2010, won the IRE award for investigative journalism. Whitaker is not totally anti-psychiatry as some people maintain. He has stated: … “It (Psychiatry) has a duty to develop selective-use protocols, which seek to minimize long-term use of antipsychotics (and other psychiatric medications). I also believe that our society should provide the resources to enable this rethinking of the drugs.”
No doubt Bipolar Disorder has been overdiagnosed. Some individuals and professionals have classified drug and alcohol abuse as “medicating an underlying bipolar disorder.” This interpretation excuses and dismisses the serious consequences of substance abuse. At the same time, it may be hooking some people into taking pills, without getting them off substances of abuse.
The “chemical imbalance” theory of mental illness has never been proven. In fact, this theory was never accepted by Psychiatry. Some people conclude that psychiatrists and pharmaceutical companies have pushed this notion in order to make money and sell pills. Today the marijuana industry is pushing marijuana for most mental health conditions, including depression, bipolar autism and ADHD in children. Unfortunately, many with schizophrenia use pot, although it makes their problems worse.
In Saving Psychiatry, Addictions Psychiatry Can Help
If Psychiatry became better at distinguishing the underlying roots of mental health issues, our treatments could be better. British journalist Patrick Cockburn writes eloquently as to why he believes his son, Henry, became schizophrenic. The diagnosis was precipitated by heavy marijuana use between the ages of 14 and 19. After years of trial and error, and Henry’s refusal to take medication, the son has been stabilized with Clozapine.
Perhaps, because of a focus on pills for insurance purposes, Psychiatry often falters, despite the DSM Manual. There needs to be better discernment of root causes. Which illnesses are a result of substance use,** or trauma, and/or a combination of both?*** Treating trauma and Adverse Childhood Experiences (ACEs) before people resort to substance abuse would bring down the number of people needing psychiatrists. However, the most adverse cases of trauma or extreme psychosis may need to be medicated, including foster children whose parents suffered from drug abuse. Even when psychiatric pills cause side effects, the alternative can be worse.
As for epidemic of Heroin, Fentanyl and opioid pill overdoses, policies focused on harm reduction have failed to stem the number of deaths by overdose. Most states have passed making it easier for doctors and law enforcement to stop the overdoses. Yet, this policy doesn’t treat the underlying addiction. Cost and insurance companies should not determine matters of mental health, or life and death.
Notes
* PTSD is very real but only professionals should diagnose it. At times, “bipolar disorder” and ADHD were also used too loosely and over-diagnosed.
**A NAMI (National Alliance for Mental Illness) Minnesota publication gives special attention to marijuana among the drugs that can cause psychosis, as well as legal drugs such as steroids and ADHD drugs. Epidemiological research of nearly 19,000 drug abusing Finnish subjects showed that marijuana most consistently led to a diagnosis of long term schizophrenia (Niemi-Pynttäri JA, Sund R, Putkonen H, Vorma H, Wahlbeck K, Pirkola SP. Substance-induced psychoses converting into schizophrenia: a register-based study of 18,478 Finnish inpatient cases. J Clin Psychiatry. 2013 74(1):e94-9).
*** Victims of PTSD who turned to marijuana with deadly results: Cascade Mall shooter Arcan Cetin, an early marijuana user with PTSD killed five people at a Macy’s in Washington. Stephen Bourgoin who recently killed five teens in a wrong way crash also suffered from childhood trauma, too. Eddie Routh was a veteran with PTSD who smoked marijuana before killing Chris Kyle and Chad Littlefield. NBC Nightly reported that Richard Rojas, the veteran who rammed into several people and killed a teen in Times Square, used marijuana before driving into the crowds.
The average medical marijuana cardholder in California is a 32-year-old male who uses it for chronic pain. If so many young people have so much chronic pain, it’s tempting to think medical marijuana is for “anyone who can fake an ache,” according to Professor Jon Caulkins of Carnegie Mellon
Two young women who wrote to Parents Opposed to Pot explained their need for medical marijuana to deal with traumatic childhoods. One said it was because her mother had committed suicide, while the other said she had experienced traumatizing sexual abuse.
Using marijuana in order to numb painful feelings, or for getting high, will only mask the underlying emotional pain. In all cases of psychological issues, including PTSD, marijuana works against true healing, no matter how much temporary relief it provides.
21st Century Strategies for Healing
Since pain or disease (dis ease) is imbalance, the body which created the disease can also be the body which heals the disease.
Dr. Libby Stuyt, a professional advisor to Parents Opposed to Pot uses Brain Synchronization Therapy to heal trauma in the body and bad memories. The neuroplasticity of the brain means that even post-traumatic experiences can be weakened or discarded. At the same time, the brain can relearn forgotten neural pathways.
Dr. Libby Stuyt is Medical Director for the Circle Program at the Colorado Mental Health Institute
Besides Brain Synchronization Therapy, Dr. Stuyt recommends both EMDR (Eye Movement Desensitization and Recovery) and Biofeedback based on heart rate variability.
Treating Root Causes Rather than Just the Symptoms
The good news is that there are ways to treat PTSD and chronic pain that don’t involve drugs, ways that treat the root causes rather than symptoms. “Medical” marijuana does not provide deep healing.
Medical marijuana is an addiction-for-profit industry which needs new users and promotes long-term use. Habitual users run the risk of becoming psychotic. Like continuous opiate users, they may also develop addiction.
At the Alternative Wellness Club, published in Oregonlive, 2014, patients were introduced to “dabbing.” Some of these users claimed to have bipolar disorder which may in fact be related to trauma–or triggered by marijuana. Dabbing increases the risk for addiction and psychosis.
The recent report from National Academy of Science found marijuana can give moderate relief to three medical conditions, pain being one of the conditions. Although the human body has cannabinoid receptors, marijuana’s cannabinoids are foreign to our bodies. They’re not endo-cannabinoids, the body’s natural occurring chemicals, but exo-cannabinoids. With marijuana use over time, THC will replace the cannabinoids associated with joy and happiness.
Therefore, it’s hard to claim THC is truly “natural” for humans.
Mind-body healing solutions are the “natural” solutions, and they cannot be addictive. They offer help for chronic suffering in ways “medical” marijuana and pharmaceutical medicines cannot help.