In 2012, Washington voters approved Initiative 502, legalizing cannabis. Back then, the black market was dominated by dried cannabis flower, with a potency of approximately 10%.
Dried cannabis flower is biologically limited to about 30% potency, and I-502 capped the potency of edibles at 10%.
But in an oversight of extraordinary proportions, there was no potency limit established for cannabis concentrates like THC-infused vape oils, shatter, and dab wax. Enter science, industry, business investors, and profit motivation and, today, concentrates with 99 percent potency are readily available at cannabis retailers.
According to researchers, these concentrates are “as close to the cannabis plant as strawberries are to Frosted Strawberry Pop-Tarts.” Cannabis concentrate sales have soared from 14% of the market share in 2015 to 37% in 2019.
I have devoted my professional and legislative career to mental health and substance use prevention, treatment, and recovery.
Spurred by reports of youth with cannabis-induced psychosis filling emergency departments and psychiatric wards and high school students having psychotic episodes after dabbing (inhaling), I began to delve into the research on cannabis and psychosis.
The literature is both definitive and damning. Washington’s leading cannabis experts at the University of Washington and Washington State University recently released a consensus statement summarizing the science:
“High potency cannabis use can have lifelong mental health consequences, which often manifest in adolescence or early adulthood. Daily cannabis use, particularly of high potency products, increases the risk of developing a psychotic disorder, like schizophrenia, and is related to an earlier onset of symptoms compared to people who do not use cannabis.”
During the 2020 legislative session, I introduced a bill to cap the potency of cannabis concentrates at 10%. This figure matched the limit for edibles and was a starting point for negotiation. The bill included an exemption for patients using high potency concentrates for medical purposes.
I had numerous meetings with cannabis industry representatives, and no one was aware of the psychosis link. Though they disagreed with my proposed solution, industry leaders were emphatic in their commitment to coming to the table as thoughtful partners to address this issue.
So, you can imagine my surprise when, instead of proposing more palatable policy solutions as promised, cannabis industry representatives testified before the House Commerce & Gaming committee that the research implicating cannabis in psychotic disorders is unfounded.
Borrowing from the well-worn playbooks of their forefathers, big tobacco and opioid manufacturers, cannabis business leaders attempted to poke holes in the science and offer alternative explanations.
In 1957, tobacco industry director Clarence Cook Little wrote: “No one has established that cigarette smoke, or any one of its known constituents, is cancer-causing to man.”
Sixty-three years later, cannabis industry leaders testified to our legislature that “cannabis use [is] not independently associated with psychosis.”
Modeling after Purdue Pharma, the opioid maker that wrote that addiction “is not caused by drugs … it is triggered in a susceptible individual by exposure to drugs,” the cannabis industry tried to offer a counter theory – that it is people who have a genetic predisposition for psychotic disorders who are developing them and then using cannabis to self-medicate.
That theory has been debunked by studies that account for family history and still show a significant increase in psychotic disorders from cannabis use.
I never anticipated the cannabis industry would enthusiastically agree to a low potency limit. I only expected them to make good on their word – to show up as earnest partners in addressing their product’s role in one of the largest emerging health crises of our time.
When the industry’s opening move is to spit on the consensus of the scientific community in the spirit of climate deniers, it’s difficult not to question the sincerity of their espoused commitment to public health.
I’ve introduced House Bill 1463, which caps the potency of cannabis concentrates at 30% and raises the age of purchase for concentrates from 21 to 25. Washington’s cannabis industry now has a second chance to act with integrity and come to the table as problem solvers.
It is only the fate of our children with which we are gambling.
Rep. Lauren Davis (D-Shoreline) serves northern King County and a portion of Edmonds in the 32nd Legislative District. She was the founding executive director of the Washington Recovery Alliance and taught UW’s graduate mental health policy course.
Attached is a list of medical articles that document medical warnings against marijuana that are running in newspapers throughout the country, to warn in advance of participation in 420 events.
Average flower is 17.1% in one state with legal sales of recreational marijuana, Colorado, much higher than the national average (HIDTA, 2017), and as high as 30% THC in some samples (NBC News report). It should be noted that variation in testing results is quite high between laboratories (Jikomes and Zoroob, 2018).
Jikomes N, Zoorob M. The Cannabinoid Content of Legal Cannabis in Washington State Varies Systematically Across Testing Facilities and Popular Consumer Products. Sci Rep. 2018 Mar 14;8(1):4519. doi: 10.1038/s41598-018-22755-2. https://www.nature.com/articles/s41598-018-22755-2.pdf
Processed cannabis reaches up to 90% THC
Jikomes N, Zoorob M. The Cannabinoid Content of Legal Cannabis in Washington State Varies Systematically Across Testing Facilities and Popular Consumer Products. Sci Rep. 2018 Mar 14;8(1):4519. doi: 10.1038/s41598-018-22755-2. https://www.nature.com/articles/s41598-018-22755-2.pdf
Marijuana is the Number 1 substance now found in Colorado suicides, 10-19 years old, 2014-2016
Causes mental illness, and is associated with onset of schizophrenia and other psychotic disorders such as bipolar disorder with psychosis
Association with schizophrenia and other psychotic disorders such as bipolar and schizophrenia. (Miller, 2017; Cougle et al., 2015), completed suicides and suicide attempts (Arendt et al., 2013; Silins et al., 2014; Clarke et al., 2014) and violence towards others (Arseneault et al., 2000; Dugre et al., 2017; Harford et al., 2018) particularly in those who develop marijuana-induced psychosis.
Arseneault L, Moffitt TE, Caspi A, Taylor PJ, Silva PA. Mental disorders and violence in a total birth cohort: results from the Dunedin Study. Arch Gen Psychiatry. 2000;57(10):979-86.
Arendt M, Munk-Jørgensen P, Sher L, Jensen SO. Mortality following treatment for cannabis use disorders: predictors and causes. J Subst Abuse Treat. 2013;44(4):400-6.
Clarke MC, Coughlan H, Harley M, Connor D, Power E, Lynch F, Fitzpatrick C, Cannon M. The impact of adolescent cannabis use, mood disorder and lack of education on attempted suicide in young adulthood. World Psychiatry. 2014;13(3):322-3.
Cougle JR et al. (2015). Quality of life and risk of psychiatric disorders among regular users of alcohol, nicotine, and cannabis: An analysis of the National Epidemiological Survey on Alcohol and Related Conditions (NESARC). J Psychiatr Res., 66-67, 135-141
Di Forti M, et al. Proportion of patients in South London with first-episode psychosis attributable to use of high potency cannabis: a case-control study. Lancet Psychiatry. 2015;2(3):233-8.
Harford TC, Chen CM, Kerridge BT, Grant BF. Self- and other-directed forms of violence and their relationship with lifetime DSM-5 psychiatric disorders: Results from the National Epidemiologic Survey on Alcohol Related Conditions-III (NESARC-III). Psychiatry Res. 2018;262:384-392.
Silins E, Horwood LJ, Patton GC, Fergusson DM, Olsson CA, Hutchinson DM, Spry E, Toumbourou JW, Degenhardt L, Swift W, Coffey C, Tait RJ, Letcher P, Copeland J, Mattick RP, for the Cannabis Cohorts Research Consortium. Young adult sequelae of adolescent cannabis use: an integrative analysis. Lancet Psychiatry 2014; 1(4): 245-318.
Starzer MSK, Nordentoft M, Hjorthøj C. (2018) Rates and Predictors of Conversion to Schizophrenia or Bipolar Disorder Following Substance-Induced Psychosis. Am J Psychiatry,175(4), 343-350
Harm to unborn, nursing babies
Marijuana harms unborn children (Jenkins et al., 2007; Trezza et al., 2012; Tortoriello et al., 2014; Grewen et al., 2015; Zumbrun et al., 2015; Leemaqz et al., 2016; Benevenuto et al., 2017), and may concentrate in breast milk if used repeatedly (Perez-Reyes and Wall, 1982; Grotenhermen, 2003), with consequences for the developing neonate (Astley and Little, 1990).
Astley SJ, Little RE. Maternal marijuana use during lactation and infant development at one year. Neurotoxicol Teratol. 1990 Mar-Apr;12(2):161-8.
Benevenuto SG et al., Recreational use of marijuana during pregnancy and negative gestational and fetal outcomes: An experimental study in mice. Toxicology. 2017 Feb 1;376:94-101
Grewen K, Salzwedel AP, Gao W. Functional Connectivity Disruption in Neonates with Prenatal Marijuana Exposure. Front Hum Neurosci. 2015;9:601.
Grotenhermen F. Pharmacokinetics and pharmacodynamics of cannabinoids. Clin Pharmacokinet. 2003;42(4):327-60. Review.
Jenkins KJ, Correa A, Feinstein JA, Botto L, Britt AE, Daniels SR, Elixson M, Warnes CA, Webb CL; American Heart Association Council on Cardiovascular Disease in the Young. Non-inherited risk factors and congenital cardiovascular defects: current knowledge: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young: endorsed by the American Academy of Pediatrics. Circulation. 2007 Jun 12;115(23):2995-3014.
Leemaqz SY et al. Maternal marijuana use has independent effects on risk for spontaneous preterm birth but not other common late pregnancy complications. Reprod Toxicol. 2016;62:77-86.
Perez-Reyes M, Wall ME. Presence of delta9-tetrahydrocannabinol in human milk. N Engl J Med. 1982;307(13):819-20.
Tortoriello G, et al. Miswiring the brain: Δ9-tetrahydrocannabinol disrupts cortical development by inducing an SCG10/stathmin-2 degradation pathway. EMBO J. 2014;33(7):668-85.
Trezza,V. et al. Altering endocannabinoid neurotransmission at critical developmental ages: impact on rodent emotionality and cognitive performance. Front Behav Neurosci. 2012; 6: 02. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3265033/
Zumbrun EE et al. Epigenetic Regulation of Immunological Alterations Following Prenatal Exposure to Marijuana Cannabinoids and its Long Term Consequences in Offspring. J Neuroimmune Pharmacol. 2015; 10(2):245-54.
Marijuana causes cyclic vomiting
Sorensen CJ, DeSanto K, Borgelt L, Phillips KT, Monte AA. Cannabinoid Hyperemesis Syndrome: Diagnosis, Pathophysiology, and Treatment-a Systematic Review. J Med Toxicol. 2017;13(1):71-87. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5330965/
Alaniz VI, Liss J, Metz TD, Stickrath E. Cannabinoid hyperemesis syndrome: a cause of refractory nausea and vomiting in pregnancy. Obstet Gynecol. 2015 Jun;125(6):1484-6.
Marijuana can trigger violence in those with PTSD and make PTSD worse
Wilkinson ST, Stefanovics E, Rosenheck RA. Marijuana use is associated with worse outcomes in symptom severity and violent behavior in patients with posttraumatic stress disorder. J Clin Psychiatry. 2015 Sep;76(9):1174-80.
Friedman A, Glassman K, Terras A Violent Behavior as Related to Marijuana and Other Drugs, by Albert Journal of Addictive Diseases, Vol 20(1), 2001,pp. 49-72. Marijuana users nearly as likely to engage in violent behaviors as crack users.
Marijuana is linked to increased driving fatalities
Staples JA, Redelmeier, DA, The April 20 Cannabis Celebration and Fatal Traffic Crashes in the United States. JAMA Intern Med. 2018;178(4):569-572. doi:10.1001/jamainternmed.2017.8298 Rate of traffic fatalities go up 12% after 4/20 festivities, in comparison to one week before and one week after.
Bosker WM, Kuypers KP, Theunissen EL, et al. Medicinal Δ9-tetrahydrocannabinol (dronabinol) impairs on-the-road driving performance of occasional and heavy cannabis users but is not detected in standard field sobriety tests. Addiction. 2012;107(10):1837-1844.
Compton WN, Volkow Nd, Lopez MF. Medical marijuana laws and cannabis use: intersections of health and policy, JAMA Psychiatry. 2017: 74 (6): 559-560
Del Balzo G, Gottardo R, Mengozzi S, Dorizzi RM, Bortolotti F, Appolonova S, Tagliaro F, “Positive” urine testing for Cannabis is associated with increased risk of traffic crashes, Journal of Pharmaceutical and Biomedical Analysis. https://doi.org/10.1016/j.jpba.2017.12.059
Ramaekers JG, Kauert G, van Ruitenbeek P, Theunissen EL, Schneider E and Manfred R Moeller, High-Potency Marijuana Impairs Executive Function and Inhibitory Motor Control. Amer Col of Neuropsychopharmacology (2006) 31, 2296–2303.
Raemakers, JG Driving Under the Influence of Cannabis: An Increasing Public Health Concern. JAMA published online March 26, 2018 Regular cannabis users wrongfully believe that cannabis does not affect their driving performance or that they can compensate for cannabis-associated impairment. Raemakers_2018 JAMA driving editorial.pdf
World Health Organization. Drug Use and Road Safety: A Policy Brief. Geneva, Switzerland: World Health Organization; 2016.
Marijuana associated with lung disease, cancer
Marijuana smoke is associated with lung disease (Tan et al., 2009; Tashkin, 2015) and the development of some cancers (Efird et al., 2004; Lackson et al., 2012). High levels of the cannabinoid receptor that is preferentially activated by THC (CB1) correspond to shorter survival in many cancers (Michalski et al., 2008; Carpi et al., 2015; Suk et al., 2016)
Carpi S, Fogli S, Polini B, Montagnani V, Podestà A, Breschi MC, Romanini A, Stecca B, Nieri P. Tumor-promoting effects of cannabinoid receptor type 1 in human melanoma cells. Toxicol In Vitro. 2017 Apr;40:272-279. doi: 10.1016/j.tiv.2017.01.018. Epub 2017 Jan 26
Efird JT, Friedman GD, Sidney S, Klatsky A, Habel LA, Udaltsova NV, Van den Eeden S, Nelson LM. The risk for malignant primary adult-onset glioma in a large, multiethnic, managed-care cohort: cigarette smoking and other lifestyle behaviors. J Neurooncol. 2004 May;68(1):57-69.
Lackson et al., 2012, Population-based case-control study of recreational drug use and testis cancer risk confirms an association between marijuana use and nonseminoma risk. Cancer 188:5374-83
Michalski CW, Oti FE, Erkan M, Sauliunaite D, Bergmann F, Pacher P, Batkai S, Müller MW, Giese NA, Friess H, Kleeff J. Cannabinoids in pancreatic cancer: correlation with survival and pain. Int J Cancer. 2008;122(4):742-50. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2225529/pdf/nihms38106.pdf
Suk KT, Mederacke I, Gwak GY, Cho SW, Adeyemi A, Friedman R, Schwabe RF. Opposite roles of cannabinoid receptors 1 and 2 in hepatocarcinogenesis. Gut. 2016;65(10):1721-32. http://gut.bmj.com/content/gutjnl/65/10/1721.full.pdf
Tan WC, et al. Marijuana and chronic obstructive lung disease: a population-based study. CMAJ. 2009;180(8):814-20
Tashkin DP. The respiratory health benefits of quitting cannabis use. Eur Respir J. 2015;46(1):1-4
Legal marijuana increases youth use (Cerda et al., 2017) and is associated with youth switching to more potent marijuana products (Borodovsky et al., 2017)
Use by youth in 8th and 10th grades has gone up significantly in Washington State (Cerda et al., JAMA Pediatrics ). School districts with the highest density of legal dispensaries in Colorado have a 30% higher rate of use in students by the time they reach their senior year of high school (Healthy Kids Colorado Survey, 2015: Adolescent Health); and to compile data on density of dispensaries for each school district https://weedmaps.com/dispensaries/in/united-states/colorado)
The percentage of youth on probation testing positive for marijuana has increased steadily since 2012 (DPS, 2017)
Borodovsky JT, Lee DC, Crosier BS, Gabrielli JL, Sargent JD, Budney AJ. U.S. cannabis legalization and use of vaping and edible products among youth. Drug Alcohol Depend. 2017; 177:299-306. https://www.ncbi.nlm.nih.gov/pubmed/28662974
Cerdá M, Wall M, Feng T, Keyes KM, Sarvet A, Schulenberg J, O’Malley PM, Pacula RL, Galea S, Hasin DS. Association of State Recreational Marijuana Laws With Adolescent Marijuana Use. JAMA Pediatr. 2017;171(2):142-149. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5365078/
Marijuana decreases IQ in those who begin their use young
Meier MH, Caspi A, Ambler A, Harrington H, Houts R, Keefe RS, McDonald K, Ward A, Poulton R, Moffitt TE. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A. 2012 Oct 2;109(40):E2657-64. doi: 10.1073/pnas.1206820109
Mj harms developing adolescent and young adult brains.
Camchong J, Lim KO, Kumra S. Adverse Effects of Cannabis on Adolescent Brain Development: A Longitudinal Study. Cereb Cortex. 2017 Mar 1;27(3):1922-1930. doi: 10.1093/cercor/bhw015. https://academic.oup.com/cercor/article/27/3/1922/3056289
Allan GM Simplified guideline for prescribing medical cannabinoids in primary care Canadian Family Physicians Vol 64: February 2018 2018 Cannabis Prescribing Guidelines.pdf.
Olfson M, Wall M Cannabis Use and Risk of Prescription Opioid Use Disorder in the United States American J Psychiatry. Cannabis use, even among adults with moderate to severe pain, was associated with a substantially increased risk of nonmedical prescription opioid use at 3-year follow-up. https://doi-org.proxy.hsi.ucdenver.edu/10.1176/appi.ajp.2017.17040413
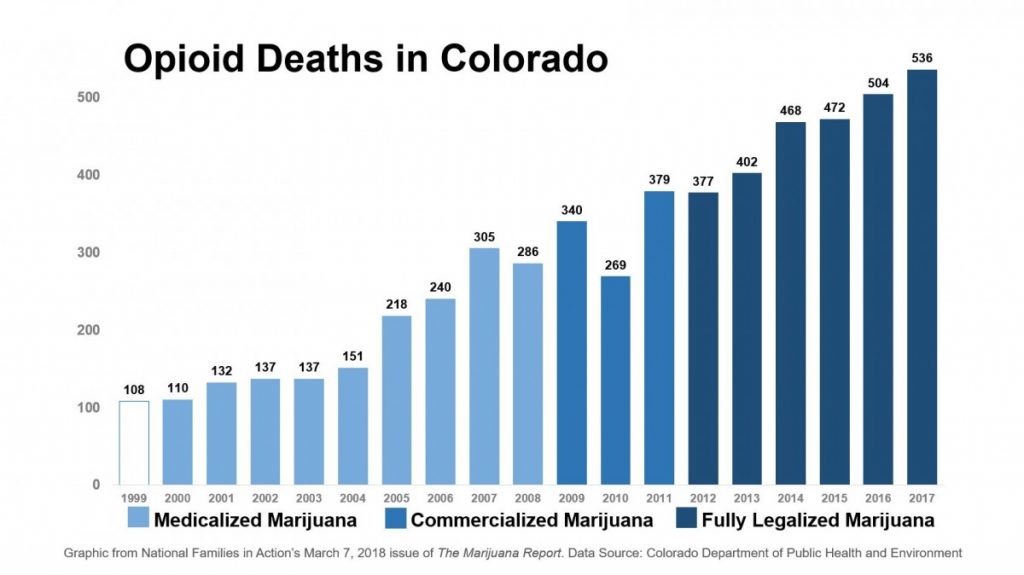
Graph provided by The Marijuana Report/National Families in Action. March 2018
Olfson M, Wall M Cannabis Use and Risk of Prescription Opioid Use Disorder in the United States, American J Psychiatry. Cannabis use, even among adults with moderate to severe pain, was associated with a substantially increased risk of nonmedical prescription opioid use at 3-year follow-up. https://doi-org.proxy.hsi.ucdenver.edu/10.1176/appi.ajp.2017.17040413