Is the Marijuana Lobby Trying to Buy Your Legislature and Your Votes?
If marijuana has a medical application that can be proven, Merck and Pfizer will probably see the benefit of getting into the 4.2 billion dollar business. Marijuana companies, like pharmaceutical companies, contribute heavily to politicians and lobbying efforts. Unlike the pharmaceutical industry, they don’t go through a rigorous testing and approval process. The marijuana industry uses pesticides, even banned pesticides, but it promotes itself as organic and natural.
Medical marijuana “caregivers” have no accountability and liability, and their lobbyists know it. We think it is wrong when the marijuana industry lobbyists give parents with very sick children false hope.
Marijuana lobbyists should not be seen as having pure and “compassionate” motives, as they pretend.* The public has a right to know that CBD for epilepsy does not always work.
A few of the children treated with an artisanal CBD (cannabidiol, the derivative of marijuana used for epilepsy) have died, and some of the children treated with cannabis oil for cancer also died.
In Montana a few years ago, Cashy Hyde’s father was featured on TV, saying his son had been cured of cancer using cannabis oil. Sadly, the boy eventually died, sometime after the startling announcement that he had been cured. The constant nurture and love from his parents probably helped to extend his life.
A man in Iowa who advocated for marijuana also died of cancer. In Australia, a little girl whose father had been treating her neuroblastoma with cannabis oil died in May. Receiving constant love, attention and kind wishes from others sent good vibes into the world, but no medical professional thought it had an effect on the cancer.
When reading about the remarkable claims advocates of medical marijuana propose, please remember the placebo effect. We don’t know why placebos cure some people and not others. It could be the power of belief, or the result of a person’s own immune system having the ability to fight the disease.
Parents Opposed to Pot objects to the tactics of marijuana lobbyists because:
They give partial truths, attempt to sway public opinion while hiding essential facts.
They engage in unfair defamation of character and advertising. Two years ago Rep. Debbie Wasserman Schultz and Rep. Andy Harris were targeted with cruel and slanderous attacks because of their votes regarding medical marijuana. Rep. Wasserman Schultz recently voted to allow veterans to be allowed marijuana — although it makes PTSD worse.
They outpsend the opposition to marijuana legalization and target youth with their advocacy, while pretending to be grass roots. Smart Approaches to Marijuana was founded after the vote to legalize in Washington and Colorado.
*The 1996 ballot in legalizing marijuana in California was called the Compassionate Use Act and people were led to believe it was only for terminally ill people with cancer and AIDS. In reality, only 3-5% of the marijuana has been used for these conditions.
(First of 2 articles on deceptive practices of the marijuana lobby/industry) Doesn’t the public have a right to know that children a so called”life-saving” product doesn’t always work.?
Informing parents that children can die after using the non-pharmaceutical CBD is not suggesting that the CBD kills; it is merely suggesting that to call it “life-saving” is misleading. Parents who have watched their children suffer much and are desperate for a cure should not be promised more than can be given. What sounds too good to be true can be too good to be true.
A family in Arizona who was part of a lawsuit to get the extracts for their son saw a dramatic difference in the boy, an improvement in all levels of functioning. Nonetheless, the poor boy died. The family still advocates for marijuana extracts. They saw their son have a better life for a period of time before his death.
One child who moved to Colorado for the CBD medication got help, but still died. The mother returned home alone. The medical marijuana industry doesn’t tell you that sometimes these “miracle cures” don’t work.
Why are People, Legislators Shielded from the Whole Truth?
Recently parents came out in droves to lobby for medical marijuana in Pennsylvania, spending the night at the state legislature. Had these parents been told that children with seizures could have participated in the trials conducted at New York University? At the time, GW was looking to recruit 150 more patients for the second part of the third phase of trials on Dravet Syndrome.
Medical marijuana campaigns don’t always supply the whole truth, especially when there’s much drama surrounding the presentation. When Dr. Sanjay Gupta went on television with his special segments about marijuana, he publicly advocated for “medical” marijuana using the example of Charlotte’s Web, an artisanal CBD product from Colorado. The televised documentaries were called Weed 1, Weed 2 and Weed 3.
At the end of Weed 3, it was mentioned that Vivian, the little girl whose family moved to Colorado for an extract of marijuana not available in New Jersey, was no longer being longer being helped as much as she had been previously. Were people listening?
Why Support Artisanal CBD?
National Families in Action (NFIA) published the American Epilepsy Society’s statements against artisanal CBD. NFIA has written about the advantages of having pharmacy-grade, FDA-approved medicine over artisanal products, which haven’t been tested for mold or pesticides and may not have the same exactitude in dosage.
Like the “Right to Know” campaign on GMOs, shouldn’t there be a Right to Know about CBD oil advocacy, or a “Right to Know about “medical” marijuana?
Parents who are considering alternative treatments for devastating diseases or conditions have a right to know that some of the experimental medicines that are aggressively promoted do not always save a child’s life. These preparations should never be called “life-saving,” because no one can prove that phrase to be true.
“Medical” marijuana has succeeded in shielding itself from lawsuits in ways that pharmaceutical companies would never be able to do.
By Robert L. DuPont, MD,President, Institute of Behavior and Health, a 501(c)3 non-profit organization working to reduce illegal drug use through the power of good ideas.
Often overlooked in discussions of drug policy today is the nature of the drug problem. The global drug problem can be traced to the innate nature of the human brain. The mammalian brain is extremely vulnerable to chemicals that stimulate brain reward. These chemicals are drugs of abuse. They produce far more intense brain reward than any natural reward, even sex and food. The repeated use of drugs of abuse leads to addiction. In its definition of addiction, the American Society of Addiction Medicine notes that it is “characterized by inability to consistently abstain, impairment in behavioral control, craving, diminished recognition of significant problems with one’s behaviors and interpersonal relationships, and a dysfunctional emotional response.”
Addiction is a chronic, often fatal, illness that typically begins in adolescence. The earlier an individual uses drugs of abuse, including alcohol and marijuana, the more likely it is that the person will develop a substance use disorder later in life. The best way to prevent addiction is to prevent the use of these substances. As a 13-year-old said to me years ago, “I don’t want to try cigarettes because I might like them.”
Modern Drug Use Epidemic
While the biology of addiction has not changed for millions of years, over the past half century drug use has changed dramatically. In the modern drug abuse epidemic, whole populations are exposed to a mind-bending array of drugs of abuse by powerful routes of administration. This has never happened before in human history.
Marijuana, the most widely used illegal drug, has been transformed in the time since the peak of its use in the United States in 1978. The potency of marijuana, as measured by the level of THC (the primary active cannabinoid in marijuana), has tripled over this time. New modes of marijuana consumption have increased the potency of marijuana delivery. For example, butane hash oil contains dramatically higher levels of THC, with concentrations up to 90 percent.
The addiction landscape also has changed as a result of the non-medical use of legal prescription drugs. Eighty percent of the global opioid supply is consumed by Americans who constitute less than five percent of the world’s population. With widespread medical use of opioid analgesics has come an epidemic of opiate dependence. The number of drug overdose deaths in the US has surpassed highway fatalities. The widespread use of prescription drugs has led to changes in the demographics of heroin use and subsequent heroin overdoses. Forty years ago heroin addiction was mostly confined to young inner-city men who often were involved in criminal activities. The new demography of heroin is the result of the demography of those that use pain medications non-medically. An estimated half of young heroin users previously abused prescription opioids prior to their heroin use. Heroin addiction has reached all parts of the country, especially small towns and rural areas, and is no longer limited to minority, male or lower income populations.
The drug epidemic continues to evolve in complex ways even as the public attitudes toward the use of drugs are shifting. Attitudes today are far more permissive toward the “recreational” use of drugs, especially marijuana. National polls indicate that a growing majority of Americans now favor legalization of marijuana for “recreational” use by adults.
Well-Funded Lobby Pushes for Marijuana Normalization
The well-funded lobby promoting the normalization of the use of marijuana (and other drugs) is based on the erroneous premise that marijuana is not only safe but also beneficial. (Ed. note: Three billionaires have spent an estimated $200,000,000 to legalize marijuana.) In contrast to this view, the science is clear that marijuana use is a serious threat to health, safety and productivity. As the negative impact of legal marijuana in the states of Colorado and Washington – and in the states that permit “medical” marijuana – is more widely understood, attitudes toward permissive drug use will shift once again.
The US, and the entire world, is at a crossroads in drug policy today with two oppositional perspectives on the future of drug policy. On the one hand is the vision on which current global drug policy was established in the first decades of the 20th century with the US in the lead which separates medical use from non-medical use of drugs with abuse potential. Under this framework, the goal of drug policy is to limit the use of drugs of abuse to medical uses only. Drugs of abuse are provided only through the process of physicians’ prescriptions and dispensed at pharmacies in a closed system and only for the treatment of diseases. The use of drugs of abuse outside of this very limited medical practice and their sale is illegal, punishable by the criminal law.
This well-established formulation of drug policy now is threatened by an alternative vision that treats drugs of abuse the way alcohol and tobacco are treated: through regulated production and sale to adults for legal use for any purpose. The campaign for this alternative drug policy begins with the legalization of marijuana but the stakes are far greater because it applies to all drugs of abuse and because there are enormous potential profits to be earned in this new marketplace. This move erases the sharp line between legal and illegal drugs. Erasing this line frustrates prevention and it opens the floodgates to widespread drug use.
Addiction Goes Up When Percent Usage Increases
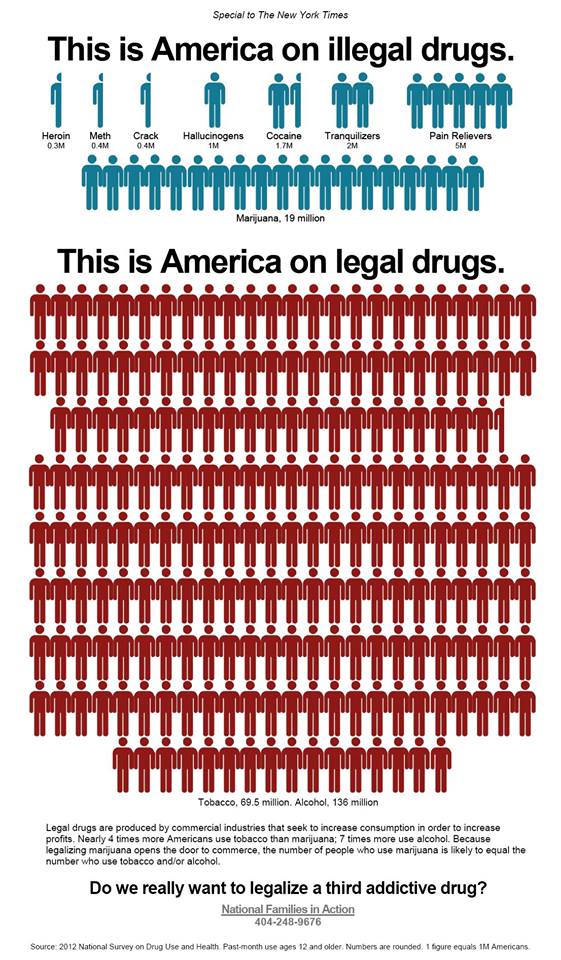
When considering the potential public health impact of the legalization of drugs of abuse, including marijuana, it is helpful to consider the rates of use of the two legal drugs. Among Americans age 12 and older, 52 percent used alcohol and 27 percent used tobacco in the past month whereas 9 percent used any illegal drug. Only 7 percent of Americans used marijuana. Treating marijuana – to say nothing of other drugs of abuse – the way alcohol and tobacco are treated most certainly will increase availability and with it dramatically increase the level of marijuana use to a level that is similar to the use of the two currently legal drugs.
Is increased marijuana use and subsequent proportional increases in marijuana addiction in the interest of the nation’s public health? I don’t think so. The use of alcohol and tobacco are the two leading causes of preventable illness and death in the United States. Adding a third legal drug will add to the devastation that these legal drugs already generate.
What is the better answer for the future of drug policy, if it is not the legalization and regulation of drugs of abuse? The future of an effective drug policy lies in finding ways to reduce the use of drugs of abuse that are compatible with modern values and laws. This search for better ways to reduce illegal drug use is the focus and the agenda of the Institute for Behavior and Heath, Inc. (www.ibhinc.org). There are many good new ideas for drug policy, all based on the recognition of the vulnerability of the brain to the excessive, unnatural stimulation of brain reward mechanism by drugs of abuse which leads to addiction for millions of people and the resulting devastation suffered by these individuals, their families and their communities.
Rather than embrace drug legalization, we must develop innovative policies and programs that reduce the use of drugs of abuse and we must provide assistance, including quality treatment that achieves long-term recovery, to those with substance use disorders.
Robert L. DuPont, M.D.
President, Institute for Behavior and Health, Inc.
Former Director, National Institute on Drug Abuse (1973-1978)
Former White House Drug Chief (1973-1977)
(Editor’s Note–Original article, “The Changing State of Drug Policy,” is reprinted with permission from the Institute of Behavior and Health website, where footnotes align exactly with text. It publishes several excellent articlesabout the influence of drug policy on addiction, drugged driving,etc.)
American Society of Addiction Medicine. (2011). Public Policy Statement: Definition of Addiction. Chevy Chase, MD: American Society of Addiction Medicine. Available: http://www.asam.org/advocacy/find-a-policy-statement/view-policy-statement/public-policy-statements/2011/12/15/the-definition-of-addiction
National Institute on Drug Abuse. (2010). Drugs, Brains and Behavior: The Science of Addiction. NIH Pub No. 10-5606. Rockville, MD: National Institute on Drug Abuse, National Institutes of Health, US Department of Health and Human Services. Available: http://www.drugabuse.gov/sites/default/files/sciofaddiction.pdf
Drug Enforcement Administration. (2014). The Dangers and Consequences of Marijuana Abuse. Washington, DC: Drug Enforcement Administration Demand Reduction Section, US Department of Justice. Available: http://www.justice.gov/dea/docs/dangers-consequences-marijuana-abuse.pdf
Manchikanti, L., Fellows, B., Ailinani, H., & Pampati, V. (2010). Therapeutic use, abuse, and nonmedical use of opioids: a ten-year perspective. Pain Physician, 13(5), 401-435. Available: http://www.painphysicianjournal.com/2010/september/2010;13;401-435.pdf
Centers for Disease Control and Prevention. (2014). Prescription Drug Overdose in the United States: Fact Sheet. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Unintentional Injury Prevention. Available: http://www.cdc.gov/homeandrecreationalsafety/overdose/facts.html
Kuehn, B. M. (2014). Driven by prescription drug abuse, heroin use increases among suburban and rural whites. JAMA, 312(2), 118-119.
Johnson, K. (2014, April 17). Heroin is a growing threat across USA, police say. USA Today. Available: http://www.usatoday.com/story/news/nation/2014/04/16/heroin-overdose-addiction-threat/7785549/
National Institute on Drug Abuse. (2013, April). Heroin. DrugFacts. Rockville, MD: National Institute on Drug Abuse, National Institutes of Health, US Department of Health and Human Services. Available: http://www.drugabuse.gov/sites/default/files/drugfacts_heroin_final_0.pdf
Cicero, T. J., Ellis, M. S., Surratt, H. L., & Kurtz, S. P. (2014). The changing face of heroin use in the United States: a retrospective analysis of the past 50 years. JAMA Psychiatry, 71(7), 821-826.
Pew Research Center. (2014, April 2). America’s New Drug Policy Landscape. Washington, DC: Pew Research Center. Available: http://www.people-press.org/files/legacy-pdf/04-02-14%20Drug%20Policy%20Release.pdf
Volkow, N.D., Baler, R.D., Compton, W.M., & Weiss, S.R.B. (2014). Adverse health effects of marijuana use. The New England Journal of Medicine, 370(23), 2219-2227.
Richter, K. P., & Levy, S. (2014, June 11). Big marijuana—lessons from big tobacco [Perspective]. The New England Journal of Medicine. Available: http://www.nejm.org/doi/full/10.1056/NEJMp1406074
Substance Abuse and Mental Health Services Administration. (2013). Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Established in 1978, the Institute for Behavior and Health, Inc. (IBH) is a 501(c)3 non-profit organization working to reduce illegal drug use through the power of good ideas. IBH websites include: www.ibhinc.org, www.StopDruggedDriving.org, www.PreventTeenDrugUse.org, and www.PreventionNotPunishment.org.